By: Dr. Ron Carlson, Dental Surgeon
Designer chemicals known as medicine-drugs-are greatly ineffective, impotent in preventing or treating disease in this day and age. We have now about 17,000 plus “diseases” defined by the medical profession as opposed to 104 maladies identified at the time of Buddha, about 2,500 years ago.
What’s happened on the way to Global Transformation? Have we lost all common sense, logic and intuition in our world? Are we so addicted to the “drug man” that we cannot break free?
The founding of the first dental school in the world was in 1840 at Baltimore, Maryland—Baltimore College of Dental Surgery. This formalization of educational training was the necessary next important step in the evolvement of the dental surgeon, the specialist of the orthopedic surgeons, the “medical men” known of in those early years of American history. Most all practitioners of the art and science of dental surgery at that time were well trained in medicine first holding a MD degree or the equivalent.
Until 1840 and the institution of the first dental school for dental surgery, there were two modes of training; the first, as a “self made” method attracting those who felt they were “prepared and ready to do all that dental art and skill could accomplish;” and the second called the “preceptor” method, for those who were nurtured, trained and taught by an existing practitioner in the art and science of dental surgery.
The advent and reasoning behind establishing a dental college independent of the existing medical college in Baltimore is contentious and convoluted by historical speculations. Some historians say Drs. Hayden and Harris—only two, but the most prominent, of many of the founders of the college of dental surgery at Baltimore—wished first for a “chair” in the medical school, thus making it a specialty of medicine like otology, rhinology, neurology—i.e. odontology chair. However, other historians speculate that a movement for an independent school from the medical school was based upon the unique needs presented by the art and science of dental surgery—that of dealing with a highly specialize area of the body requiring one skilled in all the sciences of medical practice—physiology, chemistry, anatomy, pathology—and the art of dealing with the hardest structures of the body, the odonton-complex.
Common understanding as we entered the 20th Century was that general infections of the body could generate oral infections and oral infections could do the same for the general condition. We had just witnessed a breakthrough in science showing that there was a relationship between infections and small parasites called bacteria—now we know that virus’ and prions are also involved.
An aspect of general infection theory was the focal theory of infection that asserted that “dental foci” could impact the general health of humans. That these small entities known as bacteria could migrate to other parts through the circulatory system of the body and set up foci of that infection in other organs or tissues, was well accepted by most.
Dr. Hunter of the London Fever clinic addressed the McGill graduating class in medicine in about 1910 using the term Oral Sepsis and the need to be vigilant about patients’ oral hygiene. He asserted that many chronic infectious illnesses are remedied by simply hygiene of the mouth, good nutrition, or removal of septic teeth and gums, our dental hardware too.
Louis I. Grossman DDS called the father of modern endodontics wrote about oral focal infections impacting general health. Publishing in the Dental The Cosmos in 1925 page 1150—1155, Focal Infection and Its Oral Significance he added to the theory greatly by stating:
“The manner of transmission of bacteria from a primary focus of infection is usually hematogenous and sometimes lymphagenous. The microorganisims confined in the focus of infection may reach the blood circulation by way of the capillaries, thereby gaining systemic access; especially is this true of organisims with a preference for high oxygen tension, such as Streptoccus viridens. At other times the metastasis is by way of the lymph channels.”
Later in his 1940 text, Root Canal Therapy, Grossman minimized the issues about “dead teeth,” periapical infections by stating:
“Despite the inherent weakness of such case reports (during the 19th early 20th Century), it cannot be denied that periapical infection can, and sometimes does, cause infection elsewhere in the body, or that it may contribute to ill health. The frequency with which such infections exist and causes systemic disease, is open to question, however, and has without a doubt been greatly overemphasized in the past.”
Reading the full paper of 1925 and his comments in the first edition in 1940 of his text gives a sense of the historical shift away from Oral Sepsis to the justification of so-called “modern root canal therapy,” a license for leaving gangrenous tissues in the human jawbones.
Like the great amalgam-mercury controversy of the early 1800s (Amalgam Wars), Shatz’s Proteolysis-Chelation theory of decay dissolving enamel, not just the lone acid theory (later justifying fluoride in our water supplies as a preventive measure) and the focal theory of infection were fundamentally voted out of the profession in the mid 1940s by the IADR and the ADA.
What was not recognized in the last Century was that the chemical effluent being dissolved and released into the general circulatory system by the root canalled dental organ in the jaw, its degradations products (much like those of a dead rat under the bed) are composed of very toxic thioethers, and cadavarene and purtracene the breakdown products of putrefaction—protein decomposition.
 The new computer tomography imaging discloses a more precise structure of the internal anatomy of teeth conveying the true relationship of the internal anatomy to the periodontal ligament and bone. In the 20th Century the canals depicted in Figure 1 were thought of as straight lines ending at the tips of the roots. This was errant, as we now know. The red areas in Figure 1 show that communications with the ligament about the tooth are more plentiful and robust. What is not shown here is the fact that the dentine is filled with dental lymph intercommunicating with the surrounding periodontal ligament, bone and marrow through lateral canals in the dentine. We offer Figure 2 as a representation of that fact that teeth are porous and sweat outwardly.
The new computer tomography imaging discloses a more precise structure of the internal anatomy of teeth conveying the true relationship of the internal anatomy to the periodontal ligament and bone. In the 20th Century the canals depicted in Figure 1 were thought of as straight lines ending at the tips of the roots. This was errant, as we now know. The red areas in Figure 1 show that communications with the ligament about the tooth are more plentiful and robust. What is not shown here is the fact that the dentine is filled with dental lymph intercommunicating with the surrounding periodontal ligament, bone and marrow through lateral canals in the dentine. We offer Figure 2 as a representation of that fact that teeth are porous and sweat outwardly.
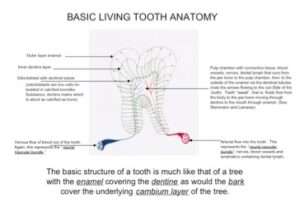
Figure 2.
Beyond these fact, adding to the dilemma that now confronts us is that we know for certain many of the disinfectants to clean the pulp chamber, root canals, and their micro-canals used by the endodontist are cytotoxic and mutagenic. The discussions and clarification of these factors never happened in the 20th Century due to the narrow window from which one viewed the issue before the profession, thus leading to the denial for the remainder of the Century of the deleterious impact of leaving dead teeth in the human jaw after root canal therapy.


Figure 3.
Enter the new designer drugs (weapons) developed during WW II and a shift to the designer chemicals that would solve our world problems in the areas of health, diet and nutrition, ending hunger, and on it goes. If a root canal tooth is infected (which all are) the course or action in modern endodontic treatment is analgesics, antibiotics, antipyretics or anti-inflammatory drugs. We still languish in the last century paradigm (LCP), outmoded.
In the USA, we knew nothing about acupuncture and energetic health. Today we know a bit more but the (LCP) prevails due mostly to fake news and fake education.
The focal theory of dental sepsis has made a strong final appearance and is beginning to be accepted as a Principle in our understanding. It will prevail due to its veracity. Yes, they equivocate but tepidly.
I give an example. A current text used in education, Oral Microbiology at a Glance (RJ Lamont et al) 2010 speaks volumes in acknowledging the role of root canal therapy—Endodontic Infections—and dental implants-Peri-implantitis-in systemic illnesses, as well as that of general periodontal disease. The text verifies the fact that these practices can be readily implicated with the cause of systemic toxic infectious conditions.
Big Pharma keeps pumping out new designer chemical and our people get sicker. These products prevent the symptoms but avail no one of a cure—a return to their natural state of health.
For the past about thirty-five (35) years the author has accumulated data on odontons (dental organs called teeth), which for one reason or another had to be removed. Most of these dental organs were dead, “cadavered,” having had “root canals.” However, the sample presented here is for the past three decades includes 317 reports (about 358 dead teeth) with root canal fillings (and ~19 people with failed dental implants, total implants ~30). In most every case there was an inflammatory, infected, or degenerate condition (reactive bone lesions), often with actinomycotic organisms, (observed 45-50% of the time) that was identified by a board certified pathologist from Queens Hospital Pathology Department.
The summation of these findings is sorted out in the following table:
HISTO-PATHOLOICAL STUDIES 1986-2017 OF SOFT TISSUE & BONE ABOUT THE ROOTS OF ENDO TEETH AND METAL IMPLANTS DONE AT QUEENS HOSPITAL HONOLULU, HAWAII
| Gender | Age | Endo Tooth # | Pathology | Bacteria |
|---|---|---|---|---|
| Female 11/3/17 | 42 | 19 | Periapical granuloma/abscess…marked acute/chronic inflammation with reactive bone | (-) Actinomyces |
| Female 9/26/17 | 62 | 30 Pre-Endo | Periapical granuloma/cyst, acute/chronic inflammation, reactive bone | (-) Actinomyces |
| Female 8/29/17 | 41 | 19 Pre-Endo | Periapical granulation tissue/fibrosis, acute chronic inflammation, “partially necrotic bone” (dead bone) | (+) Actinomyces |
| Female 8/26/17 | 79 | 27/28 | Periapical granuloma/cyst, marked acute chronic inflammation, reactive bone | (+) actinomyces |
| Male 7/27/17 | 66 | 2 | Periapical granuloma, marked acute chronic inflammation, reactive epitheilium (cyst) | (+) actinomyces |
| Female 7/26/17 | 40 | 3 | Periapical granuloma, fibrosis, chronic inflammation, radicular cyst reactive bone | (+) Actionmyces |
| Female 7/15/17 | 63 | 3,5 | Periapical granuloma/cyst, fibrous tissue, chronic infection with reactive bone | (+) Actionmyces |
| Female 5/20/17 | 68 | Titanium Implant #29 Abscess on mental foramen -83uA | Periapical granuloma/abscess, marked chronic inflammation, necrotic bone | (+) Actionmyces |
| Male 5/19/17 | 68 | 18 | Periapical abscess/granuloma, marked acute/chronic inflammation, necrotic bone | (+) Actinomyces |
| Male 12/1/16 | 29 | 8,9,10 | Periapical abscess/granuloma , marked acute chronic inflammation | (+) Actinomyces |
| Male 11/13/16 | 54 | 13 | Periapical scar, fibrosis | (-) |
| Female 11/11/16 | 54 | 18, 19 | Radicular Cyst, granulation fibrosis with marked acute/chronic inflammation and reactive bone | (-) |
| Male 9/26/16 | 65 | 19 | Periapical Granuloma/Cyst acute choronic inflammation, reactive bone | (+)
|
| Female 8/27/16 | 88 | 19 | Periapical Granuloma Cyst, marked acute chroinic inflammation, reactive bone | (+) Actinomyces |
| Male 7/14/16 | 52 | 3 | Radicular Periapical Cyst, acute/chronic inflammation, granulation/fibrous tissue. | (+) Actinomyces |
| Female 7/9/16 | 55 | 13 | Radicular Periapical Cyst, marked acute / chronic inflammation, massive granulation tissue and reactive bone. | (+) |
| Female 6/23/16 | 75 | 20 | Radicular Periapical Cyst, granulation fibrous tissue, chronic inflammation | (-)
|
| Female 5/10/16 | 67 | 18 | Periapical Granuloma (abscess) with marked acute chronic inflammation | (+)
|
| Female 2/29/16 | 66 | 18 | Radicular (Periapical) Cyst, cystic lesion with granulation tissue and marked acute chornic inflammation | (-)
|
| Male 2/16/16 | 72 | 18/19 | Radicular Cyst, granulation fibrous tissue acute/chronic inflammation. | (-) |
| Female 2/15/16 | 57 | 18/19 | Fibrosis/ Reactive bone lesions | (-) |
| Female 1/28/16 | 60 | 5 | Squamous Mucosa with acute and chronic inflammation | (-) |
| Female 1/8/16 | 60 | 4 | Periapical radicular cyst, granulation tissue acute/chronic inflammation | (+) |
| Female 11/12/15 | 52 | 9 | Periapical fibrosis/scar, acute/chronic inflammation, reactive bone lesions | (-)
|
| Female 11/2/15 | 56 | Metal implant #4 (with sinus perforation) -63 uA | Fibrosis, chronic inflammation, reactive bone lesions | (-) |
| Female 11/2/15 | 56 | 29,30,31 | Periapical Granuloma, chronic inflammation, reactive bone lesions | (-) |
| Female 10/24/15 | 33 | 8,9 | Periapical Granuloma/Cyst, marked acute chronic inflammation, necrotic bone | (+) |
| Female 10/24/15 | 33 | 4,5 | Periapical Granuloma/Scar, chronic inflammation, reactive bone lesions | (-) |
| Female 8/31/15 | 60 | 13 | Periapical Granuloma, Cyst chronic inflammation, inflamed mucosa | (+)
|
| Female 8/28/15 | 48 | 29 | Periapical Granuloma/Cyst, marked acute/chronic inflammation, fibrosis, necrotic bone | (-)
|
| Female 8/27/15 | 33 | 2,3 | Periapical Granuloma/Cyst, marked acute/chronic inflammation, fibrosis, reactive bone | (-)
|
| Male 7/31/15 | 64 | 3 | Periapical Granuloma, fibrosis, marked chronic inflammation` | (-) |
| Female 7/28/15 | 35 | 29 | Peripaical/Radicular Cyst/Granuloma Acute/chronic inflammation, reactive epithelium, reactive bone | (+) |
| Female 7/16/15 | 46 | 15 | Periapical Radicular Cyst/Granuloma Chronic inflammation, reactive epithelium, reactive bone | (-) |
| Female 6/18/15 | 61 | 31 | Periapical Radicular Cyst, marked acute/chronic inflammation, reactive bone, fibrosis | (+) |
| Male 6/13/15 | 77 | 3,4 | Periapical granuloma/cyst, marked acute/chronic inflammation, reactive bone | (+) |
| Female 6/3/15 | 67 | 12 | Periapical granuloma, marked chronic/acute inflammation | (-) |
| Female 5/28/15 | 61 | 14 | Periapical scar, chronic inflammation, reactive bone | (-)
|
| Female 5/26/15 | 59 | 18/19 | Periapical Granuloma/Cyst, marked acute chronic inflammation, reactive bone | (-) |
| Female 5/9/15 | 54 | 3 | Periapical Granuloma/Cyst, acute chronic inflammation | (+)
|
| Female 4/23/15 | 64 | 29 | Periapical Granuloma/Cyst, acute/chronic inflammation | (+)
|
| Female 4/17/15 | 69 | 19 | Periapical Granuloma, acute/chronic inflammation, “devitalized bone” dead bone | (-) |
| Female 4/14/15 | 61 | 2 | Periapical Granuloma, acute/chronic inflammation, reactive bone | (-)
|
| Female 3/21/15 | 73 | 10 | Periapical Granuloma, acute/chronic inflammation | (-) |
| Female 3/19/15 | 68 | 10 | Radicular (Periapical) Cyst, granulation tissue with fibrosis, acute / chronic inflammation, reactive bone | (-) |
| Male 3/10/15 | 35 | 19 | Radicular (Periapical) Cyst, granulation tissue with fibrosis, acute/chronic inflammation | (-) |
| Female 2/2/15 | 69 | Metal Implant #29/30 area -45 uA | Periapical granuloma (prei-implantitis, acute/chornic inflammation, reactive bone | (-) |
| Male 1/31/15 | 86 | 2 | Radicular (periapical) cyst, acute/chronic inflammation, reactive bone | (+) |
| Female 1/29/15 | 69 | 5, 3 | Reactive and Devitalized (dead) bone | (+)
|
| Male 1/19/15 | 27 | 13 | Periapical Granuloma, fibrosis, acute/chronic inflammation, reactive bone | (+) |
| Male 1/16.15 | 86 | 18 | Periapical Granulma/Cyst, fibrosis, acute/chronic inflammation, reactive bone | (-)
|
| Female 1/10/15 | 83 | 31 | Periapical Granuloma/Cyst fibrosis, acute/chronic inflammtion | (-) |
| Male 1/9/15 | 63 | 9 | Periapical Granuloma/Cyst, fibrosis, acute/chronic inflammation | (+)
|
| Female 1/6/15 | 71 | 7 | Periapical Granuloma/Scar, fibrosis, acute/chronic inflammation | (-) |
| Female 12/22/14 | 70 | 3 | Periapical Granuloma/Cyst, fibrosis, marked acute/choronic inflammation, reactive bone | (+)
|
| Male 12/17/14 | 40 | 30 | Periapical Granuloma/Cyst, Chronic inflammation, fibrosis, reactive bone | (-) |
| Female 12/17/14 | 43 | 19 | Radicular (Periapical) Cyst, marked acute/chronic inflammation, fibrosis, granuloma | (+)
|
| Female 12/7/14 | 70 | 15 | Periapical Granuloma/Cyst, mareked chronic and acute inflammation | (-) |
| Female 11/7/14 | 70 | 12 | Periapical Granuloma, marked acute/chronic inflammation,reactive bone | (-)
|
| Female 11/5/14 | 73 | 3 | Radicular Cyst (Periapical) acute/chronic inflammation, fibrosis, reactive bone | (+) |
| Male 10/7/14 | 65 | Zirconia Implant Posts #18 and #19 area | Periapical Granuloma with pus, marked acute/chonic inflammation with fibrosis and reactive bone | (+)
|
| Female 10/1/14 | 82 | 18 | Periapical Granuloma with pus, marked acute/chronic inflammation with fibrosis and reactive bone | (-) |
| Male 9/26/14 | 65 | Ziconia Implant Post #30 and #29 area | Periapical Granuloma, marked acute/chronic inflammation… | (+)
|
| Male 8/21/14 | 70 | Titanium Implant Posts # 9 | Peridental Fibroma / Scar, chronic inflammation, dead bone | (-) |
| Male 8/14/14 | 51 | 14 | Periapical Granuloma, acute/chronic inflammation, reactive bone | (-) |
| Female 8/14/14 | 66 | 29,31 | Periapical Granuloma / Scar, Chronic Inflammation reactive bone | (-) |
| Male 8/8/14 | 70 | 14, 15, 16 | Periapical Granulomas, marked acute/chronic inflammation, dead bone, fibrous tissue | (+)
|
| Male 7/28/14 | 70 | 30 | Periapical Granuloma, chronic inflammation, reactive bone | (-) |
| Female 6/26/14 | 23 | 9 | Periapical Granuloma/Scar, Fibrosis, chronic inflammation with reactive bone | (-) |
| Female 6/22/14 | 77 | 4 | Periapical Granuloma/Cyst, granulation/fibrous tissue, marked acute/chronic inflammation | (+)
|
| Female 6/22/14 | 64 | 6 | Periapical Scar, chronic inflammation, reactive bone | (-) |
| Female 6/16/14 | 80 | 14 | Periapical Abscess/Granuloma, marked acute/chronic inflammation, Necrotic Bone | (+)
|
| Female 6/16/14 | 80 | 12 | Periapical Abscess/Granuloma, marked acute/chronic inflammation, Necrotic Bone | (+) |
| Male 6/12/14 | 34 | 29 | Periapical Cyst/Granuloma, marked acute/chronic inflammation Reactive Bone | (-) |
| Female 6/5/14 | 66 | 3 | Radicular Cyst (Periapical) marked acute chronic inflammation, granulation/fibrous tissue Osteonecrosis (dead bone) | (+) |
| Female 5/21/14 | 44 | 9 | Periapical scar/fibrosis, reactive bone | (+) |
| Female 5/13/14 | 64 | 30 | Focal Osteonecrosis, necrotic bone, reactive bone, squamous mucosa | (+) |
| Male 5/5/14 | 34 | 18 | Periapical granuloma, chronic inflammation, fibrosis, reactive bone, degenerated bone (dead bone) | (-) |
| Female 4/22/14 | 59 | 18 | Periapical granuloma/scar, mild chronic inflammation, reactive bone | (-) |
| Female 4/19/14 | 68 | 7 | Radicular (Periapical) Cyst, granulation/fibrous tissue with marked acute and chronic inflammation, reactive bone | (+) |
| Male 4/7/14 | 47 | 14 | Periapical Granuloma Cyst, granulation/fibrous tissue with marked acute/chronic inflammation, Dead Bone | (-)
|
| Female 4/4/14 | 64 | 3 | Radicular Periapical Cyst, granulation/fibrous tissue, marked chronic/acute inflammation, Dead Bone | (-) |
| Female 4/4/14 | 49 | 14 | Periapical Granuloma/Cyst, granulation/fibrous tissue with chronic inflammation | (-) |
| Female 3/21/14 | 42 | 10 | Periapical Granuloma/Abscess, marked acute/chronic inflammation with fibrosis and granulation tissue, Dead bone, reactive bone consistent with “osteomyelitis” | (-)
|
| Male 3/11/14 | 57 | 14, 15 | Periapical Cyst/Granuloma, marked acute/chronic inflammation, Reactive Bone | (+)
|
| Female 2/22/14 | 66 | 6 | Periapical abscess/granuloma, marked a/c inflammation, Partially dead and reactive bone | (+) |
| Male 2/4/14 | 70 | 18,19 | Cystic Granuloma/marked acute-chronic inflammation, Reactive Bone | (-)
|
| Female 1/24/14 | 43 | 10 | Cystic Granuloma/ tissue with marked inflammation, Chronic and Acute Reactive Bone | (-) |
| Male 1/14/14 | 61 | 4 | Periapical scar/fibrosis, Osteonecrosis (Dead Bone) Patient has bowl cancer—this tooth #4 and two others #12 & #19 on the same meridian were root cadavers. CA dx 6mo ago | (+) |
| Male 1/13/14 | 63 | 29 | Periapical granuloma/scar, AC Inflam, dead dentine/cementum, numerous Actinomyces /Candida | (+) Candida 1st (Actinomyces) |
| Male 1/11/14 | 34 | 30 | Periapical granuloma, AC inflammation, Reactive bone, fibrosis | (-) |
| Female 12/7/13 | 44 | 2 | Periapical abscess/scar Reactive/Necrotic(dead) bone and fibrous tissue | (+)
|
| Female 11/21/13 | 66 | 28 |