The Disturbance Field Mouth-Jaw Area
By Dr. Franz Hopfer
From Neural Therapy, Reflex Zones and Somatotopies: A Key to the Diagnostic and Therapeutic Understanding of Man’s Ills, a seminar guide compiled by the American Academy of Biological Dentistry, June 1989
The disturbance-fields of the head are known to present a very broad influence in causing illnesses, and in our experience, the tooth-jaw area dominates. Therefore, the intent of my elaborations lies in trying to acquaint you with focal pathology of the tooth and its holding apparatus. To be sure, it is clear to me that for this purpose, great practical experience is also needed, on the one hand, in the evaluation of the x-ray pictures; on the other hand, in the inspection of the mouth.
Daily living shows that you are largely dependent on the cooperation and understanding of the dentist. The same goes for evaluations by the radiologist. But precisely in the field of focal-detection, many divergent opinions and interpretations prevail. The reason for this lies in the clinical development which hardly touches this territory. When it is touched upon, there are unclear and antiquated imaginations regarding the focus-happening, and frequently, an illness-causing distant effect of the teeth is made out to be absurd.
The dentist holds to that which has been lectured to him, and continues to be so during his training, seminars and graduate courses. These are dogmas which issued from the beginnings of the focus-lore and which are rigidly maintained. This condition will change only when the school will examine the modern images and concepts about disturbance field focus problems. Until then, you are obliged to orient yourself sufficiently about a specialty that is unfamiliar to you, obliged to know even more than the dentist regarding the focus-pathology of the tooth-jaw area if you do not wish to continue treating your patients in many ways only symptomatically. You may succeed in bringing a change in this unsatisfactory condition through clarifying orientation.
Another factor must not be overlooked: the attitude of patients. They generally find in the dentist a welcome comrade in the area of keeping up their teeth. They do not merely see a relevant expert in him, but they tell of practical examples from among their acquaintances who had their teeth removed but no healing came about. These objections cannot be ignored; they are too frequent. BUT, when one goes to the bottom of the matter, one sees that either only a partial sanitation was done and further devital teeth, root remnants and remaining foci are still in the jaw or, as is almost always the case, one had not even looked for other disturbance fields but had trusted in good luck regarding the assumed scapegoat.
Neural therapy offers the possibility of a causal connections diagnosis. Thereby, the value or uselessness of intended surgery can be seen in advance and you can, therefore, work in an extremely targeted way. Because, as useless as treatment of a disturbance field-dependent illness is with neglect of the disturbance field, it is exactly as useless to attempt a healing of an illness that is NOT focus-conditioned through focus therapy. To understand the focal effect of a tooth, one must realize the histologic situation. According to Pischinger every inflammation happens in the interstitial, soft cells of the connective tissue, which is distributed throughout the body. This soft connective tissue contains nerves and their endings, and it is being supplied with nutrients and oxygen via the also present vessels. It is provable that NO nerve end and no blood vessel is connected with the organ-cell itself, but they are always surrounded by connective tissue cells. In Illustration 1, you see the dentin, crossed by fine, parallel-running canaliculi, in which are found all elements of the soft connective tissues: vessels, capillaries, vegetative fibers and lymph vessels.
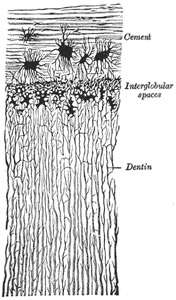
These canaliculi move to the border of the dentin-cement, but they do not end there, as is partly still being taught….[T]hese canaliculi are, via the so-called cross-connections, in contact with the surrounding bones and, thus, in metabolic exchange with the entire organism. The DEVITAL TOOTH IS THEREFORE ONLY NERVE-DEAD BUT NOT BIOLOGICALLY DEAD. Were it otherwise, it would be a foreign body and, as such, it would be expelled by the organism.
Seen in this way, also the question regarding the focus’ effective, ill-making agency, whether bacterial or abacterial toxins, or allergies, etc., is a question of secondary rank. Also, the argument of dentists – that an exact root-filling or a root-tip resection along with the removal of a granuloma is a meaningful focal-therapeutic measure – is immediately to be rejected on the basis of these histologic factors. The trimmed tooth will continue to remain in connection with all parts of the organism via the cross-connections and the soft connective tissue. Then, ONLY the extraction of such a tooth can eliminate the focus-factor and bring success.
On the granuloma, which is generally searched for in the focus-search, the following is to be said: It represents a defense measure of the reactive organism toward the stress substances of the devital tooth, can therefore be found only with a nerve-dead tooth and is not the expression of particular focus capacity.
But not only the devital or periapically changed tooth is to be considered as potential disturbance field resp. focus but a whole number of pathologic changes in the tooth and jaw area, which you find listed below. I will pick out from among them the foreign bodies and the restostitis because they are less known.
Odontogentic Focal Possibilities
- Not fully filled root canal
- Non-tightly filled root canal
- Incompletely and non-tightly filled root canal
- Complete and dense root filling
- Widened periodontal split (Periodontitis chronica plastica)
- Alveolar compacta: a) not thoroughly pursuable; b) noticeably intensified
- Diffused periapical focus
- Limited periapical focus: a) sickle-shaped; b) hood-shaped; c) lense-shaped; d) cherry core-size; e) plum core-size
- Cysts
- Fausse Route with empty canal remnant – lateral clearing
- Projecting filling with interdental bone construct
- Septum dystrophy without recognizable cause (possibly gingivitis)
- Septum changes in the sense of a paradontosis: a) horizontal atrophy; b) vertical atrophy
- Inter-radicular septum processes (anatomy of bifurcation)
- Root remainder in the antrum
- Foreign body inclusion submucous or in bone spongiosa: a) metal density (possibly amalgam); b) seemingly cement; c) of Guttapercha density
- Root remainder in the toothless jaw ledge
- Restostitides
- Ostitis around baby tooth coat
- Baby tooth remainder
- Tooth sprout (organism, seed, germ – ?)
- Impacted or half-impacted tooth
- Tilted tooth
- Dental luxation
- Tooth fracture
- Dentio difficilis
- Root tip resection
- Residiv after resection
- Mortal amputation: a) interdental focus without seeable x-ray change; b) periapical focus
- Root resorption with living tooth
- Tooth with lowered vitality
- Paradentopathies
- Diverse metals in the mouth
The foreign bodies may be of metallic or non-metallic sources. The metallic foreign bodies are recruited from amalgam remnants, which are occasionally incorporated in extraction wounds, from broken-off root treatment instruments and, in rare cases, from shell-splinters. Non-metallic foreign bodies stem from root treatment materials and non-metallic fillings. But also, diverse mouth metals (amalgam, gold, steel) can, in the acid mouth milieu, lead to measurable battery effects (up to 800 millivolt) and cause illnesses, according to disposition, through foreign energy or corrosion.
I want to emphasize in detail the Restostitis, a pathologic change in the empty jaw, also called restating Ostitis, which has been given special consideration as a focus only in recent years. The diagnosis is made from the x-ray pictures. It is often difficult because these changes are often vaguely delimited, and they are recognizable only by the washed out bone structure and a mild shading. Occasionally, the covering mucous membrane is discolored and the bone is pressure-sensitive. If it is superficially located, it is occasionally possible, after preceding anaesthesia, to break into the bone with a thin probe. Of course, the removal is only possible by surgery, whereby the bone is wide open. One finds mushy, sometimes even pussy tissues, which must be removed from the hard, healthy bone tissue with a sharp spoon and fraise. Almost always, it is more extended than expected from the x-ray picture. Histologically, one finds the picture of an inflammation. The cause is not entirely clear for the restating Ostitis. Besides a secondard healed-up extractions wound, the possibility is quite strong that it is the result of an arsenic inlay from possibly years back. The arsenic is laid on the open pulpa for devitalization and left there for three days. But because thereby it reaches by the Foramen apicale into the surrounding bone, it can continue its necrotic effect there.
This periapical irritation shows up frequently by tap-sensitivity of the tooth: that is, a mild periodontitis, 2-3 days after the [arsenic] application. It fades away quickly; in the course of years, the diffused remnants of arsenic lead to diffused necroses in the jawbone with the picture of vague demarcation (even if the tooth has long ago been removed).
The reason for my detailed elaborations on these restostitic changes is that they are barely noted by the dentist or radiologist. As already mentioned, they are not easily recognized and, moreover, are known at all only to those searching for foci. But according to our experience and notation, they are frequently found in 25% of our patients, and I consider that alarming. In seven years, we have discovered 1100 such cases in our ambulance activity, which were subsequently also confirmed by our jaw surgeon macroscopically, and by the pathology department of the Hanusch Hospital histiologically. And moreover – and this is what’s most important – they were to a high percentage the cause of other illnesses.
One chapter which remains unclear regarding a cause is the retro-molar space of the lower jaw, which has been pointed to by Sollman, Munich. Here, too, there is a pathologic change not so rarely noted, which looks similar to Restotitis and can act as a disturbance field….
From these elaborations, it becomes clear that, besides a complete x-ray status involving all teeth and toothless jaw portions, also a clinical inspection of the oral cavity is required. It must consider gum diseases, tooth pockets, fistula, sensitivity to pressure on jaw areas, and the submandibulary glands, and often uncertainties can be cleared up only by a vitality test. For this reason, the findings of the radiologist are only incomplete, and the positive cooperation of the dentist in the diagnosis, but especially in the therapy, is mandatory.
Of course, one cannot expect the dentist to pronounce whether the discovered pathologic changes actually constitute the cause of an illness. Most methods of focus diagnosis only give hints about the organ reactions at a particular place but do not reveal anything about any disease-causing distant effects. This is the very domain of Neural Therapy, with the help of which we gain a very reliable picture of distant effects, which may take their start from the most diverse organs, such as tonsils, liver, adnexes, scars, etc. One exception to this is only the odontogenic realm, not only regarding the required time of only 8 hours (compared to double the time with all other organs) to reach the desired freedom from complaints, but also regarding reliability. Only in about half of the cases in which the dentogenic realm is the source for the disease is it possible to reach a positive Huneke phenomenon. This is an experiential fact, which Ferdinand Huneke has already pointed out. When the dental test is negative, the patient who is already not too eager for sanitization will hardly agree to an adontogenic focus therapy.
We have structured our working-procedure on these factualities. First, all anamnestically established disturbances in the patient will undergo the Huneke test. If the test is negative, then we propose the radical odontogenic sanitization without testing the tooth-jaw area, just on the basis of the exclusion process. We have obtained very satisfactory results thereby. With diseases of the kidneys, the blood-forming apparatus, serious heart ailments, the condition of heart-infarction and inflammatory eye diseases we make an exception in that we begin the focus-clearing in the dentogenic sector.
Not to be forgotten is the need to explain to the patient sufficiently that after a dental sanitization no more root treatments are to be performed or else there will be the danger of the return of the complaints. Also to be mentioned are the environmental diseases of the teeth, which also diminish only after the dentogenic focus therapy. Among them is the “sensitive throat” with tonsillectomies, the tendency to lateralis medullae spinalis pharingitis. The same goes for the scars of tonsillectomy if they are a proven disturbance field and there is no permanent success after several infiltrations. With tonsillectomy, the filter station for the lymphatic drainage of the teeth is eliminated; they touch on the scars and make them a disturbance field. Therefore, BEFORE the intended removal of the tonsils, there should ALWAYS be a dentogenic sanitization performed. Usually, this makes the tonsillectomy superfluous because in the absence of stress, the chronic tonsillitis will fade away. With our large number of patients, we have at the most two tonsillectomies per year.
The second area which tends to be impaired through closeness are the nasal sinuses. In chronic, but also in acute sinusitis max. and the pansinusitis, and especially when there is therapy resistance, one is forced to think of the teeth. Not only do the root tips of premolars and the molars lie very close to the base of the jaw cavities, but they often protrude into the jaw cavity. This stress situation is caused by devital teeth and can also be seen endoscopically. These “sinusitis comitans” can, of course, only be relieved by corresponding extraction.
It is also to be considered that an odontogenic sanitization should happen under “stray protetion” because of the possible exacerbation of the distant illness. The prior administration of Elpimed along with an antibioticum and antiallergicum has proven itself well with us. Thereby, surgical difficulties are also reduced to a minimum.
The success of the sanitization follows only after elimination of ALL involved teeth and jaw-portions, and generally only weeks after the consolidation of the wounds. Often one experiences in a patient a phase of improvement or total freedom from complaints [after which he] slowly returns to his old ill health again. Then, an after-treatment is required. It consists of injections with a neural therapeuticum into the sanitized areas, in local neural therapeutic treatment of the afflicted places and in a general mood-change therapy. For this, we use Elpimed, the Paul’sche Cutivaccine or also the Ponndorf inoculation – and therewith we achieve in most cases the stabilization of the sanitization success.
In conclusion, I want to show you a case which, on the one hand, shows instructively and free from subjective statements of the patient, the success of sanitization and, on the other hand, demonstrates how serious, yes, how life-threatening, the effects of a focus can be:
On a 51 year old engineer, G.J., a panmyelopathy was diagnosed by a well-known out-of-town hemologic department. Later, he was accepted in the department of Prof. Fleischhacker and treater with Prednisolon, antibiotica and blood transfusions. There was a temporary improvement, then the blood panel values again dropped significantly. Now, two devital teeth were extracted, one week apart. Already after the first extraction, the patient felt subjectively better, and he reduced the Prednisolon doses on his own. The leucocytes rose moderately. After the second extraction, the values fell again but then rose to 5000. Likewise, the anaemia and thrombocytopenia improved so that all therapy was discontinued. In the following weeks, not only the blood panel normalized but also the leucocytes-phosphatase index and the marrow report. Since then, for over nine years, all reports remained normal, although the patient had no further treatments whatsover.
Originally published in German